Article Text

Abstract
Background Two randomized trials have evaluated clipping and coiling in patients with ruptured aneurysms. Aggregated evidence for management of ruptured and unruptured aneurysms is missing.
Objective To conduct a meta-analysis evaluating clinical outcome after aneurysm treatment.
Methods PubMed, Cochrane Central Register of Controlled Trials, and Clinicaltrials.gov were searched for studies evaluating aneurysm treatment. The primary outcome measure was an independent clinical outcome (modified Rankin scale 0–2, Glasgow Outcome Scale 4–5, or equivalent). Secondary outcomes were poor outcome and mortality. ORs were calculated on an intention-to-treat basis with 95% CIs. Outcome heterogeneity was evaluated with Cochrane's Q test (significance level cut-off value at <0.10) and I2 (significance cut-off value >50%) with the Mantel–Haenszel method for dichotomous outcomes. A p value <0.05 was regarded as statistically significant.
Results Searches yielded 18 802 articles. All titles were assessed, 403 abstracts were evaluated, and 183 full-text articles were read. One-hundred and fifty articles were qualitatively assessed and 85 articles were included in the meta-analysis. Patients treated with coiling (randomized controlled trials (RCTs)) had higher independent outcome at short-term follow-up (OR=0.67, 95% CI 0.57 to 0.79). Independent outcome was favored for coiling at intermediate and long-term follow-up (RCTs and observational studies combined—OR=0.80, 0.68 to 0.94 and OR=0.81, 0.71 to 0.93, respectively). Independent outcome and lower mortality was favored after coiling in unruptured aneurysms (database registry studies) at short-term follow-up (OR=0.34, 0.29 to 0.41 and OR=1.74, 1.52 to 1.98, respectively).
Conclusions This meta-analysis evaluating clinical outcome after coiling or clipping for intracranial aneurysms, indicates a higher independent outcome and lower mortality after coiling.
- Aneurysm
- Coil
- Hemorrhage
- Intervention
Statistics from Altmetric.com
Introduction
Subarachnoid hemorrhage (SAH) accounts for approximately 5% of all stroke cases, often occurs in a younger population than for acute ischemic stroke, and may lead to significant morbidity.1 The most common cause of SAH is a ruptured intracranial aneurysm with an overall incidence of nine per 100 000 person-years, which increases with age.2 Prevalence of unruptured aneurysms on MRI screening has been estimated to be 1.8%.3 Fatality in SAH is high4 and the risk for rupture of an untreated intracranial aneurysm increases with size and location.5
Treatment of intracranial aneurysms is based on their exclusion from the intracranial circulation to prevent bleeding, which can be achieved by surgical or endovascular techniques. Evidence suggests that coiling may be better than clipping for treatment of ruptured aneurysms for short-term and intermediate follow-up, but the generalizability has been questioned.6 A limited number of randomized controlled trials (RCTs) comparing surgical clipping and endovascular coiling of ruptured intracranial aneurysms have been carried out. One RCT was conformed in accordance with the Consolidated Standards of Reporting Trials criteria for a scientifically conducted randomized controlled trial (CONSORT)—the International Subarachnoid Aneurysm Trial (ISAT).7 Recently, 18-year follow-up data from ISAT8 were published, as well as 6-year follow-up data from the randomized Barrow Ruptured Aneurysm Trial (BRAT).9 No RCT has evaluated surgical clipping and endovascular coiling for unruptured aneurysms, and such a study is unlikely to occur since a long follow-up would be required to detect differences in outcome. Treatment of unruptured aneurysms relies heavily on the results from the International Study of Unruptured Intracranial Aneurysms (ISUIA) trial.5 An increasing number of non-randomized observational studies with short- and long-term follow-up have been published, with discordant results.
Several meta-analyses comparing clipping and coiling have been published; however, only the Cochrane review published in 2005 analyzed results for the intention-to treat population.10 The meta-analysis published by Lanzino et al11 compared the outcome of ruptured cerebral aneurysms after clipping or coiling and was based on 1-year follow-up data from three RCTs with a study population of 2732 patients. A meta-analysis by Li et al12 compared the outcome of ruptured intracranial aneurysms after clipping or coiling; searches were made until 2012, and included 13 studies with 6555 patients with 1-year follow-up, and three studies including 1845 patients with long-term follow-up. Recently, Ruan et al13 conducted a meta-analysis of unruptured aneurysms comparing patient outcome after clipping or coiling. In their study, however, the searches identified only 366 articles, seven of which met the inclusion criteria, with four studies finally being evaluated showing no significant differences for clinical outcome.13 No systematic meta-analysis including the recently published studies presenting long-term clinical outcome, and no comprehensive meta-analysis including ruptured and unruptured aneurysms stratified for follow-up time and study design, has been published.
This meta-analysis aimed to compare clinical endpoints (patient outcome and mortality) after surgical clipping or endovascular coiling of ruptured and unruptured cerebral aneurysms rather than surrogate endpoints such as occlusion patency, rebleeding, vasospasm, hydrocephalus, and re-treatment rates. Primary outcome measure was good clinical outcome (independent patient) and secondary outcome measures were poor clinical outcome (dependent patient) and mortality. As this study aimed to assess the data for both ruptured and unruptured aneurysm treatment, RCTs and non-RCTs were included in the analysis.
Given the high prevalence of cerebral aneurysms and the severity of the disease they may cause, an updated comprehensive meta-analysis of the treatment of intracranial aneurysms is needed.14
Methods
Search strategy and selection criteria
A systematic literature search was performed for studies of intracranial aneurysm treatment, surgical clipping, and endovascular coiling.
One researcher performed the literature search (AlFD), in which data were retrieved from the following databases: PubMed, the Cochrane Central Register of Controlled Trials, and the National Institutes of Health Clinical Trials, from date of inception until 10 August 2015. The following search terms were used in combinations: coiling, clipping, intracranial, randomized, endovascular, long-term, aneurysm, treatment. In order to ensure a broad search we did not use Mesh terms. Published articles were considered for inclusion. The meta-analysis was performed according to Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA)15 and Meta-analysis Of Observational Studies in Epidemiology (MOOSE).16 Institutional review board approval was considered exempt since we included only previously published articles.
Study selection and data extraction
The following inclusion criteria were used:
Randomized controlled trials;
Non-randomized studies including database registries comparing clipping and coiling with at least 10% of the study population in each treatment arm;
Ruptured or unruptured intracranial aneurysms;
Independent outcome/poor outcome and/or mortality;
Patients of any age;
English, Spanish, and Swedish studies;
Any study date;
Intracranial aneurysm location in the anterior and/or posterior circulation.
Exclusion criteria were:
Other treatments than straightforward clipping or coiling—for example, clipping in combination with bypass surgery, stent-assisted coiling, or flow-diverter treatment. Single patients were excluded if their outcomes were reported separately;
No presentation of outcomes separately for ruptured and unruptured aneurysms;
Carotid-ophthalmic aneurysms, since they do not exclusively have an intracranial localization.
Two researchers (AnfD and AIFD) independently assessed the retrieved articles and extracted the data according to a prespecified protocol into tables. Disagreements were solved by discussion. Primary outcome measure was an independent functional outcome defined as modified Rankin scale (mRS) 0–2,17 or Glasgow Outcome Scale (GOS) 4–5.18 Occasionally, if only mRS 0–1 or 0–3 was reported, this was used as definition of an independent outcome. In some studies other outcome measures were used, which were used if they were translatable into a good or poor outcome as defined above. For example, database registries present ‘discharge to home, which has been shown to correlate with mRS score 0–2 at discharge.19
Secondary outcomes were poor clinical outcome and mortality. Poor outcome was defined as mRS 3–6, GOS 1–3, or equivalent. Quality of the studies and risk of bias was assessed based on components of study design and data presentation, and extracted into tables.
Outcome data were prespecified to be stratified into three main groups according to follow-up time: short term (discharge–3 months), intermediate (>3 months–1 year), long-term (>1 year) for ruptured and unruptured aneurysms. Outcome data from RCTs, observational studies, and database registries were analyzed.
Statistical analysis
The meta-analysis was undertaken using Review Manager statistical software (RevMan, V.5.3. Copenhagen, Nordic Cochrane Centre, Cochrane Collaboration, 2014). RCTs were analyzed according to the intention-to-treat principle; observational studies were analyzed according to the post hoc analysis. Data from patients lost to follow-up in the RCTs were imputed with mRS=5 in order not to overestimate the treatment effect in studies with a higher percentage of drop-outs. Study data were pooled according to treatment allocation into surgical clipping or endovascular coiling. Outcome heterogeneity was evaluated with Cochrane’s Q test (significance level cut-off value at <0.10) and I2 (significance cut-off value >50%). The Mantel–Haenszel method was used for dichotomous outcomes with fixed or random effect (DerSimonian and Laird20) according to outcome heterogeneity. ORs with 95% CIs were calculated for all outcomes. An overall estimate for all study types was obtained only if there was no significant interaction among the different studies, defined by Higgins I2>50 and Cochrane's Q test <0.05. Assessment for publication bias was performed where appropriate (>10 studies in the same comparison) through visual inspection of funnel plots for asymmetry. Corrections for asymmetry were performed according to the trim and fill method.21 Prespecified sensitivity analyses for different outcome measurements were performed. A p value <0.05 was considered statistically significant.
Results
Searches identified 18 802 studies. 403 abstracts were assessed for eligibility and 183 articles underwent full-text evaluation. One hundred and fifty articles were included in the qualitative assessment. Major reasons for exclusion were the following: redundant cohorts presented in several publications, outcomes not stratified into ruptured and unruptured aneurysms, studies including only carotid-ophthalmic segment aneurysms, and outcomes not stratified for treatment. Eighty-five studies,5 ,7–9 ,22–98 met inclusion criteria and were included in the meta-analysis (see online supplementary figure S1). The tabulated studies included a total of 225 772 patients. The total study group of patients with ruptured aneurysms consisted of 117 495 individuals (2918 patients from RCTs, 11 303 patients from observational studies and 103 274 patients from database registry studies). The study population of unruptured aneurysms consisted of 108 277 patients (7487 from observational studies and 100 790 from database registry studies). Region of origin for included studies were Asia (n=25), Australia (n=3), Europe (n=30), USA and Canada (n=32). A full description of included studies is presented in table 1. Risk of bias and quality assessment, funding, and additional baseline parameters are presented in online supplementary table S1. Raw data tables of variables used in the meta-analyses are presented in online supplementary table 2 (ruptured aneurysms) and online supplementary table S3 (unruptured aneurysms).
Meta-analysis of ruptured aneurysm comparing coiling and clipping (short-term to long-term follow-up, OR for a functional outcome <1 favors coiling, OR for adverse outcomes >1 favors coiling)
Supplementary figure
Supplementary tables
Ruptured aneurysms
Short-term follow-up (discharge–3 months)
Three RCTs, 21 observational studies and three database registry studies were included for short-term follow-up (table 2). No major differences in baseline characteristics between the RCTs were found, except for a higher proportion of aneurysms in the anterior circulation in ISAT. No significant differences in baseline characteristics were found in the observational studies. Calculated odds ratio (RCT) for an independent functional outcome (mRS 0–2, GOS 4–5, or equivalent) after endovascular coiling compared with surgical clipping was OR=0.67 (95% CI 0.57 to 0.79, OR <1 favors coiling). The proportion of patients with a good clinical outcome after aneurysm treatment was 61% in the coiling group and 52% in the clipping group with an absolute risk reduction of 9% (95% CI 5% to 13%). The corresponding analyses for observational and database registry studies did not reach significance (OR=1.12, 95% CI 0.83 to 1.52) and (OR=1.02, 0.87 to 1.18). Mortality did not differ between the two treatment modalities in RCTs (OR=1.09, CI 0.79 to 1.50) or observational studies (OR=0.76, 95% CI 0.50 to 1.15), whereas mortality was significantly lower after surgical clipping in database registry studies (OR=0.88, 95% CI 0.80 to 0.96, OR <1 favors clipping). When all study types were combined, the overall estimation of mortality in conjunction with aneurysm treatment favored clipping (OR=0.84, 95% CI 0.72 to 0.98) with an absolute risk reduction of 1.72% (95% CI 1.31% to 2.4%) and a number needed to treat (NNT) of 59.
Intermediate follow-up (>3 months–1 year)
Four RCTs and 24 observational studies were included. Among observational studies, 72% of the studies had higher Hunt and Hess/World Federation of Neurological Societies/Fisher grade in the coiling group, whereas 12% of the studies had higher values in the clipping group, p=0.0001. The proportion of patients from the RCTs intention-to-treat population with an independent functional outcome was 74% after coiling and 66% after clipping (OR=0.69, 95% CI 0.59 to 0.81, OR <1 favors coiling). The proportion of patients with an independent functional outcome in the observational studies was 80% in the coiling group, and 78% in clipping group (OR=0.82, 95% CI 0.71 to 0.97). An interaction test showed no heterogeneity. An overall estimate for all study types favored coiling (OR=0.80, 95% CI 0.68 to 0.94, figure 1) with an absolute risk reduction of 5% (95% CI 2.91% to 7.17%) and a NNT of 20 (95% CI 13.9 to 34.4). There were no significant differences in mortality between the two treatment modalities. A higher proportion of patients undergoing surgery had a poor outcome (28%) compared with coiling (24%), p=0.04. The overall risk estimate from the RCTs and the observational studies showed an increased risk for a poor outcome in the clipping group, OR=1.26 (95% CI 1.07 to 1.48, OR >1 worse outcome after clipping).

Meta-analysis of patients treated for ruptured intracranial aneurysms having an independent outcome comparing surgical clipping and endovascular coiling in the intermediate follow-up (3 months–1 year). Forrest plot demonstrates that coiling yields a higher proportion of patients with an independent outcome compared with clipping.
Long-term follow-up (>1 year)
Two RCTs and nine observational studies were included. Baseline characteristics did not differ between treatment groups (p=0.60). For long-term follow-up, a higher proportion of coiled patients had a good clinical outcome (42%) compared with the clipped patients (37%) in the RCTs intention-to-treat population (OR=0.80, 95% CI 0.69 to 0.94). OR for a good functional outcome in the observational studies was 0.84 (95% CI 0.63 to 1.10). Long-term overall estimate from RCTs and observational studies favored coiling (OR=0.81, 95% CI 0.71 to 0.93, figure 2), with an absolute risk reduction of 4.4% (95% CI 1.30% to 7.51%). There was no difference in mortality between the two treatment arms.
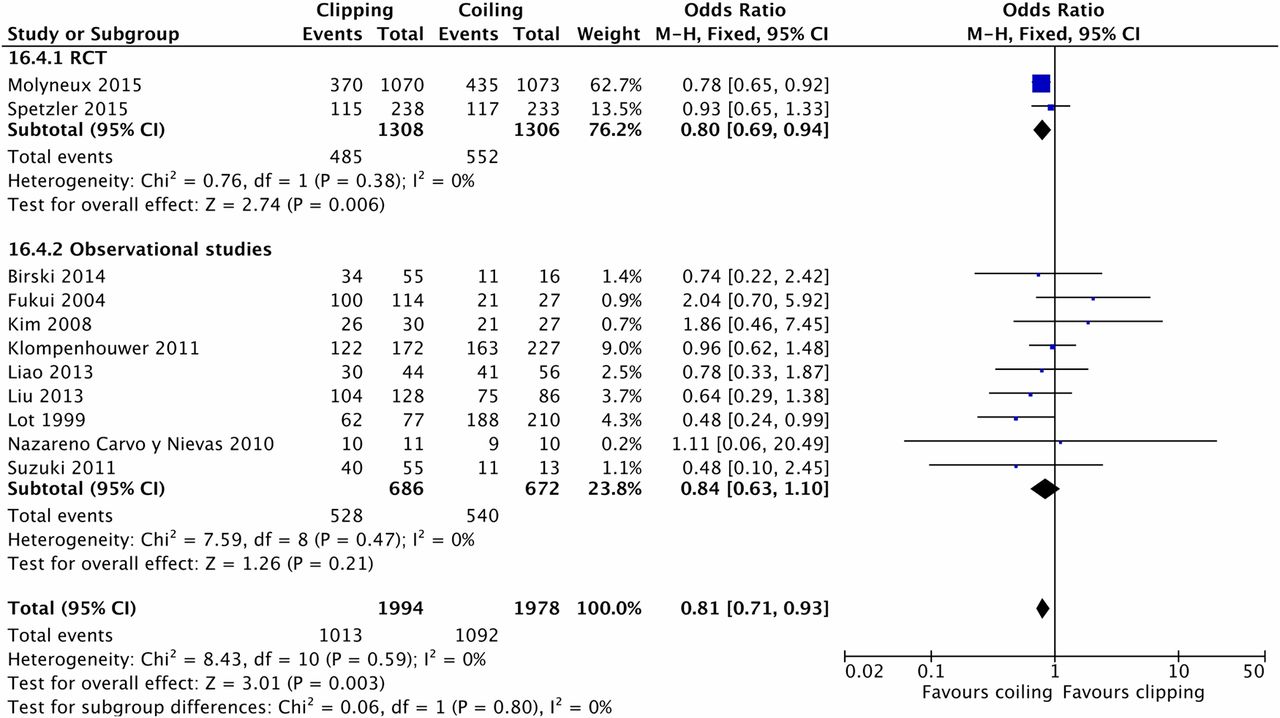
Meta-analysis of patients treated for ruptured intracranial aneurysms having an independent outcome comparing surgical clipping and endovascular coiling in the long-term follow-up (>1 year). Forrest plot demonstrates that coiling yields a higher proportion of patients with an independent outcome compared with clipping.
Sensitivity analysis
Adjusting for imbalances in baseline characteristics led to a non-significant result for short-term mortality. Sensitivity analysis for intermediate follow-up (3 months–1 year) and long-term follow-up (>1 year) did not change the summary OR.
Publication bias
Asymmetric funnel plots were observed for short-term follow-up in observational studies for good and poor functional outcomes. Adjustments for this asymmetry did not change the pooled estimate.
Unruptured aneurysms
Short-term follow-up (discharge–3 months)
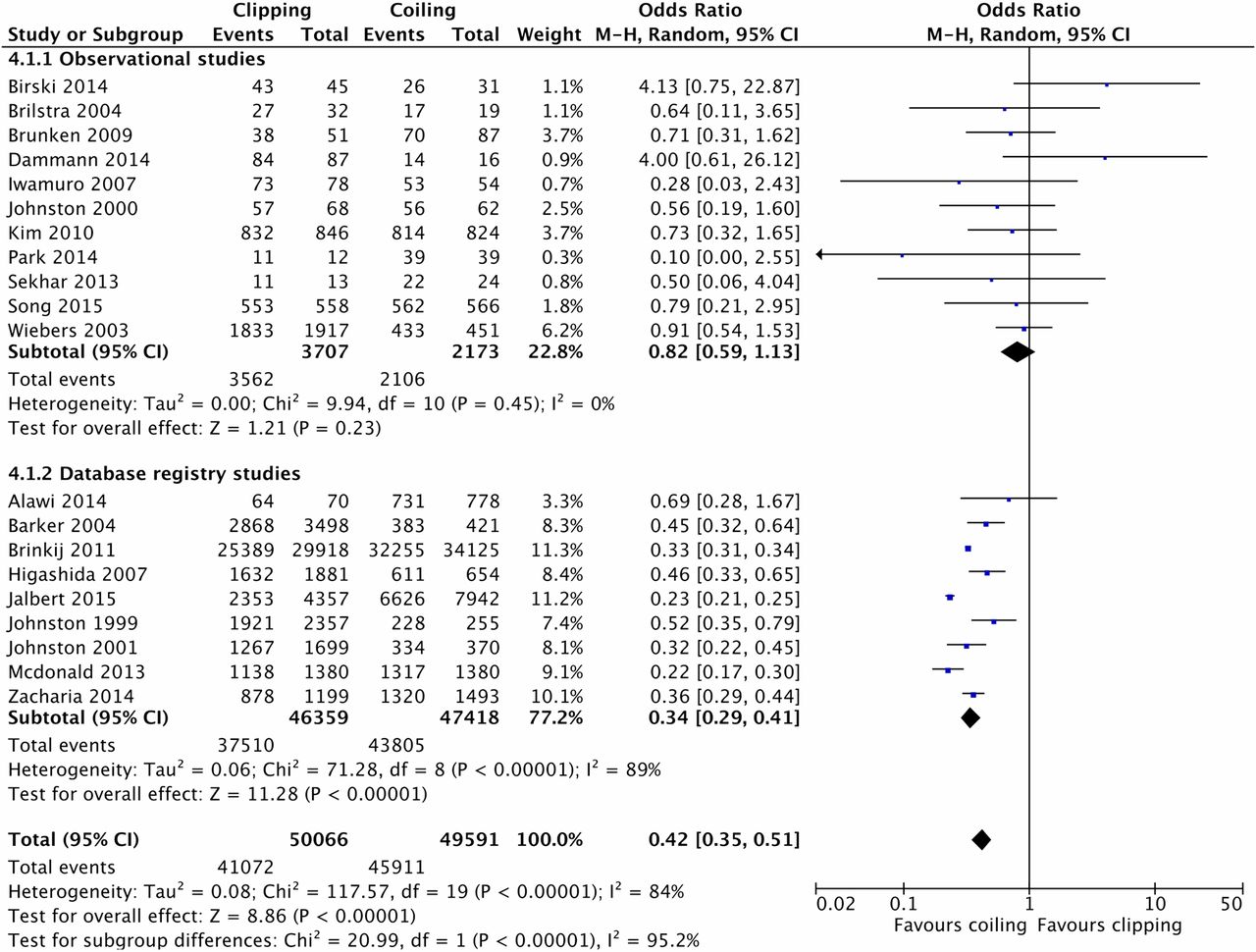
Twelve observational studies and nine database registry studies were included (table 3). The proportion of patients in the observational studies with a good functional outcome was 97% and 96% after coiling and clipping, respectively, with an OR=0.77 (95% CI 0.56 to 1.07, OR <1 favors coiling). In database registry studies, the proportion of patients with a good functional outcome was 92% after coiling and 81% after clipping, OR=0.34 (95% CI 0.29 to 0.41, figure 3), with an absolute risk reduction after coiling of 11.8% (95% CI 11.37% to 12.23%). The calculated OR for mortality in observational studies was 0.88 (95% CI 0.48 to 1.62). Short-term mortality from database registry studies favored coiling 1.74 (95% CI 1.52 to 1.98) with an absolute risk reduction of 0.68% (95% CI 0.55% to 0.82%) and a NNT of 147 (95% CI 122 to 183).
Meta-analysis of unruptured aneurysm comparing surgical clipping and endovascular coiling (short-term to long-term follow-up, OR for a functional outcome <1 favors coiling, OR for adverse outcomes >1 favors coiling)

{kind=link}
{kind=link}
{kind=link}
Meta-analysis of patients treated for unruptured intracranial aneurysms having a favourable outcome comparing surgical clipping and endovascular coiling in the short-term follow-up (<3 months). Forrest plot demonstrates in database registry studies that coiling yields a higher proportion of patients with an independent outcome compared with clipping.
Intermediate follow-up (>3 months–1 year)
Eleven observational studies were included. Pooled estimates were non-significant for all outcomes.
Long-term follow-up (>1 year)
Five observational studies were included. A good functional outcome was favored after clipping (OR=3.01, 95% CI 1.14 to 7.99, OR >1 favors clipping) with an absolute risk reduction of 2.63% (95% CI 0.46% to 4.80%). Long-term mortality after microsurgical clipping and endovascular coiling, respectively, was 0.45 (95% CI 0.09 to 2.33) based on six observational studies and 0.96 (95% CI 0.78 to 1.18) based on two database registry studies.
Sensitivity analysis
Sensitivity analysis for long-term follow-up for unruptured aneurysms changed results to non-significance 2.68 (95% CI 0.84 to 8.54) between coiling and clipping for a good/poor functional outcome.
Publication bias assessment
An asymmetric funnel plot was observed for short-term follow-up in the observational studies, with a skewness to the left. Adjustments for this skewness did not change the pooled estimate.
Discussion
This meta-analysis demonstrates a better outcome for patients treated with coiling (RCTs) for all follow-up periods, supported by the overall estimate from randomized and non-randomized studies (intermediate and long-term follow-up). At short-term follow-up, there were significantly higher mortality rates in the clipping group in the database registry studies (n=93 777). The long-term follow-up for a functional outcome in unruptured aneurysms favored clipping. However, three of five studies did not report baseline parameters, therefore these studies were excluded from the sensitivity analysis and the results were non-significant; thus we consider these results as less robust.
In the meta-analysis by Lanzino et al,11 which included three RCTs, the authors demonstrated a favorable outcome for the 1-year follow-up for ruptured aneurysms, which is consistent with our study including RCTs and observational studies. The meta-analysis performed by Li et al12 assessed the 1-year outcome for ruptured aneurysms, but found no differences among observational studies for a favorable outcome. However, for long-term follow-up based on three studies they reported a favorable outcome for coiling. The meta-analysis by Ruan et al13 did not detect any difference in mortality or proportion of patients with a favorable outcome between coiling and clipping
Aneurysmal subarachnoidal hemorrhage is treated to prevent rebleeding, with the obvious risk of further patient deterioration, and not to improve patient outcome. The outcome of the patient is multifactorial, depending on the severity of the initial bleed and also on the effectiveness and safety of the chosen treatment. Instead of choosing surrogate endpoints such as occlusion patency, rebleeding, vasospasm, and hydrocephalus, which do not necessarily reflect the clinical outcome, we chose to study clinical endpoints, such as independency, dependency, and mortality, since these are the factors most important for patients and their relatives.
The main limitations of this pragmatic meta-analysis are due to the scarcity of well-conducted RCTs.
In this meta-analysis we aimed to present results based on clinical practice and therefore included non-randomized studies and studies from database registries. There is, in general, a good correlation between randomized and non-randomized studies.99 It might be argued that if analyses with different levels of evidence reached the same conclusion this might be indicative of the generalizability of the results from the RCTs, despite methodological differences. In this study, data from different study types were pooled only when no significant interactions existed, as described previously.100
Non-randomized studies are more likely to introduce a selection bias, in which elderly and poor-grade patients are more frequently allocated to endovascular treatment. Observational studies rarely report on eligible patients not included in the study, patients lost to follow-up, or those with primary crossover to another treatment.
We used funnel-plots to explore the potential role of publication bias among the included studies. We detected an asymmetric funnel plot for observational studies in unruptured aneurysms for short-term follow-up, favoring coiling, with higher treatments effects in smaller studies. In addition, we observed a discrete asymmetric funnel plot for short-term follow-up in ruptured aneurysms, favoring clipping. This might be explained by publication bias, suggesting that studies with non-significant results favoring clipping and coiling in the ruptured and unruptured aneurysms were not published. We cannot out rule the possibility that studies on new coiling therapy are more likely to have been published than studies of conventional clipping. An explanation of the publication bias in this meta-analysis is the non-inclusion of unpublished data and the use of language restrictions.
Another limitation is due to the rapid development of endovascular techniques. Today, many aneurysms, especially unruptured ones, are treated with stent-assisted coiling as well as with intrasaccular and extrasaccular flow diverters. As primary coiling, sometimes with balloon assistance, remain the mainstay for ruptured intracranial aneurysms in many institutions, it might be argued that the results from this study provide more up to date information about ruptured than unruptured aneurysms. The panorama, for both efficacy and safety, has probably changed with the development of new techniques and tools as compared with pure coiling.
Aneurysm morphology and location, but also the clinical status and preferences of the patient, are keys in treatment decisions. Some aneurysms are regarded as difficult, and perhaps even impossible, to treat endovascularly, whereas others are feared to carry a high morbidity and mortality when chosen for open surgery. This incongruity, in that anatomical and patient-related variables make a certain treatment modality suitable, differs between coiling and clipping, making comparisons difficult. Based on results from RCTs it is unclear which patients would benefit more from clipping or coiling. True comparisons are difficult to achieve in observational studies, since treatment decisions depend on local circumstances and may vary throughout the study period. When these facts are taken into account, it can be seen that poor-grade patients were more often selected for coiling in the included studies.
A strength of our study is the thorough search of all published data in the field, especially as, to the best of our knowledge, no large RCTs comparing the outcome from coiling versus clipping are planned.
Patients receiving endovascular treatment for ruptured intracranial aneurysms have a higher proportion of good functional outcome than those undergoing clipping. There was no statistical heterogeneity for intermediate and long-term follow-up between randomized trials and observational studies and an overall estimate was obtained, making this generalizable to clinical practice, under the condition that it is technically feasible to coil the aneurysm. Data from large database registries show that patients treated with coiling have a higher proportion of good functional outcome after endovascular coiling and lower mortality, than those undergoing microsurgical clipping.
In conclusion, this is the most comprehensive meta-analysis for treatment of ruptured and unruptured intracranial aneurysms, including RCTs, observational studies, and database registry studies, stratified into short-, intermediate, and long-term outcome and shows better functional outcome after endovascular coiling than with surgical clipping.
References
Footnotes
Contributors AlFD and AnFD contributed equally to this study. AlFD and AnFD planned the work and were responsible for data collection, analysis and interpretation, and writing of the manuscript. TA interpreted the data and critically revised the manuscript. All authors approved the final version and agreed on the integrity of the work.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.