Article Text

Abstract
Objective To assess the effect of routinely delivered home-based end-of-life care on hospital use at the end of life and place of death.
Design Retrospective analysis using matched controls and administrative data.
Setting Community-based care in England.
Participants 29 538 people aged over 18 who received Marie Curie nursing support compared with 29 538 controls individually matched on variables including: age, socioeconomic deprivation, prior hospital use, number of chronic conditions and prior diagnostic history.
Intervention Home-based end-of-life nursing care delivered by the Marie Curie Nursing Service (MCNS), compared with end-of-life care available to those who did not receive MCNS care.
Main outcome measures Proportion of people who died at home; numbers of emergency and elective inpatient admissions, outpatient attendances and attendances at emergency departments in the period until death; and notional costs of hospital care.
Results Intervention patients were significantly more likely to die at home and less likely to die in hospital than matched controls (unadjusted OR 6.16, 95% CI 5.94 to 6.38, p<0.001). Hospital activity was significantly lower among intervention than matched control patients (emergency admissions: 0.14 vs 0.44 admissions per person, p<0.001) and average costs across all hospital services were lower (unadjusted average costs per person, £610 (intervention patients) vs £1750 (matched controls), p<0.001). Greater activity and cost differences were seen in those patients who had been receiving home nursing for longer.
Conclusions Home-based end-of-life care offers the potential to reduce demand for acute hospital care and increase the number of people able to die at home.
- Home care
- Hospital care
- Terminal care
Statistics from Altmetric.com
Introduction
Improving the quality of care at the end of life has become an important element in National Health Service (NHS) policy.1 Among the goals of the national strategy is a desire for people to be able to die at home or in a place of their own choosing—something that is not being achieved for everyone at present.2 Surveys consistently suggest that the majority of people would like to die or be cared for at the end of life at home.3–5 However, the proportion of people who die at home in England and Wales has been found to be lower than in some other developed countries.6 ,7 Due to the ageing population it is predicted that the annual number of deaths in England will increase by 17% between 2012 and 2030 from around 506 000 to around 590 000 deaths.8 There will either need to be a significant growth in inpatient facilities or a sharp rise in the proportion of deaths outside hospital to cope with this trend.
Palliative care at the end of life aims to prevent and alleviate symptoms, and address people's wider practical and social needs.9 There is evidence from several countries that home-based palliative or end-of-life care is associated with a higher probability of dying at home (or at least not dying in hospital).10–15 Studies also suggest that it can lead to less hospital care, lower costs and higher levels of satisfaction.13 ,16–20
However, many of the existing studies of home-based palliative and end-of-life care have been relatively small randomised trials.13 ,15 Randomised trials need to be supplemented with observational studies to assess benefits in routine settings, as the effect of the intervention can differ depending on the context in which it is delivered. Further, the characteristics of patients enrolled into trials can be different from those referred in routine practice. The available observational studies of home-based palliative and end-of-life care have compared groups of people with and without access to such services,11 ,18 ,19 without attempting to match the groups on important characteristics. This can produce misleading estimates.21 We wanted to assess if these results held for much larger samples in routine practice.
In this paper, we study the effect of a common form of home-based end-of-life care in the UK. The Marie Curie Nursing Service (MCNS), part of the Marie Curie Cancer Care charity, provides end-of-life nursing care and support to people in their own home. The service provides care to around 28 000 people annually. A small number of studies of the MCNS provided some evidence that the service is cost effective22 and that it helps a high proportion of recipients to die at home.23 However, there has been no direct comparison of people who receive MCNS care with a control group. This study set out to use larger sample sizes and a retrospectively matched control group to address the scale of impact of the MCNS model of home-based end-of-life care on hospital use and place of death.
Methods
Intervention
The MCNS is funded by NHS commissioners and donations and provides hands-on nursing care and emotional support for people in their own homes, day and night at the end of life. It aims to provide care that makes it possible for people to spend their last days of life at home rather than in hospital. Although originally it focused on caring for people with cancer, it is now available to people with other conditions. The service is provided by registered nurses and healthcare assistants, and people are referred to the service by community nursing services. The MCNS offers various models of care; however, the vast majority of people in this study were receiving the standard package of care consisting of a 9-h day or overnight shift of care.
Study cohort
The intervention group consisted of people who received MCNS care in England between January 2009 and November 2011, and who died in the same period. We excluded patients aged 18 or less, those who died in a care home and those who had not been admitted to hospital at some point between 2000 and death.
Datasets
We sourced inpatient, outpatient and emergency department data from the Hospital Episode Statistics (HES), covering all NHS-funded care provided in hospitals in England. We obtained date and place of death from the HES-linked mortality file that holds data extracted from death certificates by the Office for National Statistics.
The NHS Information Centre for health and social care (IC) acted as a trusted third party, and linked a dataset of all those who received MCNS care between January 2009 and November 2011 to HES datasets. The IC provided a pseudonymous unique identifier consistent across datasets. This method preserved participants’ anonymity by ensuring that individuals could not be identified. Further details are provided in the online supplementary appendix 1.
After data linkage by the IC, a series of cleaning steps were applied to exclude cases with missing or incomplete data. Online appendix table 1 provides further details.
Selection of controls
Controls were selected based on the same inclusion and exclusion criteria as the intervention group, but also could not have received MCNS care. A number of other exclusions were applied to the pool of possible controls before matching (see online appendix table 2).
The aim of the matching was to account for differences between patients who received MCNS care and those that did not. We aimed to select a subset of the possible controls with the same distribution of relevant characteristics as the intervention patients in the period leading up to the intervention. Ideally matched controls would have the characteristics that were used to identify cases as being eligible for MCNS care. These would include being at the end of life and considered suitable for care at home. However, these criteria do not map naturally onto variables that are recorded in HES, and so instead we used proxies. We matched cases and controls individually on a range of demographic, diagnostic and prior hospital use variables.
The matching employed a two-stage algorithm. For each case, the pool of controls was initially reduced by applying a set of exact matching criteria. These were: that controls must have died within 90 days of the case, be the same sex, be matched on recent history of cancer and not be in hospital on the index date. For each MCNS patient, the first visit date was taken as the study index date. For each possible control selected in the first stage, the index date was defined as the same point relative to death as for the intervention patient, that is, if the intervention patient had their first visit 9 days before death then the index date for the controls was 9 days before their death.
In the second stage, a single control was selected who was most similar to the case across a number of variables, using the multidimensional distance measure known as the Mahalanobis metric.24 ,25 The Mahalanobis matching included demographic variables such as age and deprivation,26 prior clinical history (recorded hospital diagnoses), and prior hospital use. One control was selected per case without replacement. The matching was assessed using the ‘standardised difference’, calculated as the difference in means across intervention and matched control groups, divided by the pooled SD. Researchers have suggested a threshold of 10% can be used to denote meaningful imbalances.27 Further details on the matching are provided in the online supplementary appendix 1.
Hospital costs
For each intervention patient and matched control we estimated their notional hospital costs in the year up to the index date and the period after until death. Hospital costs were estimated from HES data by applying the set of mandatory and indicative tariffs used in England for the reimbursement of inpatient and outpatient care (2010/2011 Payment by Results tariffs).28 Where national tariff prices were not available, 2007/2008 national reference costs (adjusted for inflation) were used. Further details on the costing method are provided in the online supplementary appendix 1.
Statistical analyses
The primary outcome measures were the proportion of people who died at home, and hospital utilisation and secondary care costs between the index date and death. We also investigated whether the impact (if any) of the intervention was affected by the time from first receiving the intervention until death.
To test the effect of MCNS care on hospital use, we constructed multivariable regression models. We performed both unadjusted analysis and analysis that adjusted for residual differences between intervention and control patients that remained after matching in terms of age, deprivation, ethnicity, number of chronic conditions, number of conditions associated with ageing, number of different cancers and prior hospital use.
For binary variables such as the proportion dying at home, we assessed differences between groups using logistic regression. Model coefficients were exponentiated to produce ORs. For ‘count’ variables such as the number of hospital admissions per head, we used Poisson regression, with coefficients exponentiated to produce the ‘incidence rate ratio’. Both the incidence rate ratio and the OR are measures of the relative impact.
The analyses of the effect of time from first receiving the intervention until death on hospital use were assessed using interaction tests. Models were constructed that included dummy variables for each of the subgroups and the interactions between the subgroup dummies and intervention status; significant differences were assumed where the CIs for the interaction term did not overlap the overall group effect.29
Hospital costs were analysed using ordinary least-squares regression. We presented differences between groups using the average predicted marginal costs, for consistency with the Poisson regression analyses of hospital use.
Ethics and governance
Research ethics approval was not required for this study as it was based on retrospective analysis using routine data. We received confirmation from the National Information Governance Board that pseudonymised patient data could be used without approval under s251 of the NHS Act 2006, and we obtained Approved Researcher status from the Office for National Statistics for mortality data.
Results
Matching
Of the 38 728 records of people who received MCNS care provided to the IC, 37 582(97%) could be linked to a pseudonymised HES identifier. The sample cases were then cleaned to remove records with errors or inconsistent data (see online supplementary appendix 1) leaving a final study group of 29 538 individuals. Overall, 78% of the MCNS cohort had a history of malignant cancer in the preceding 3 years (based on HES admitted patient records). The median time from first MCNS visit to death was 7 days (25th percentile 3 days, 75th percentile 22 days, range 0–365 days).
Before matching, the study cohort was quite different from the pool of potential controls (ie, from other patients who had died in England over the same period; see online appendix table 4). Those who received MCNS care were younger and lived in areas with lower levels of socioeconomic deprivation, but much more likely to have been diagnosed with cancer. Potential controls were much more likely to have been diagnosed with dementia or congestive heart failure, and to have had a recent history of falls and fractures.
All of the study sample could be matched to a control. After matching, the controls and intervention patients were similar in terms of a wide range of demographic, diagnostic and prior hospital utilisation variables at the index date, with no standardised differences of greater than 10% (table 1).
Standardised differences between intervention patients and controls after matching
Place of death
In all, 77% of those who received MCNS care died at home with fewer than 8% dying in hospital. By contrast, 35% of the matched controls died at home, with 41% dying in hospital (figure 1). The difference in the proportion dying at home was statistically significant (unadjusted OR 6.16, 95% CI 5.94 to 6.38, p<0.001). After adjustment, the difference remained statistically significant (adjusted OR 6.97, 95% CI 6.71 to 7.25, p<0.001).
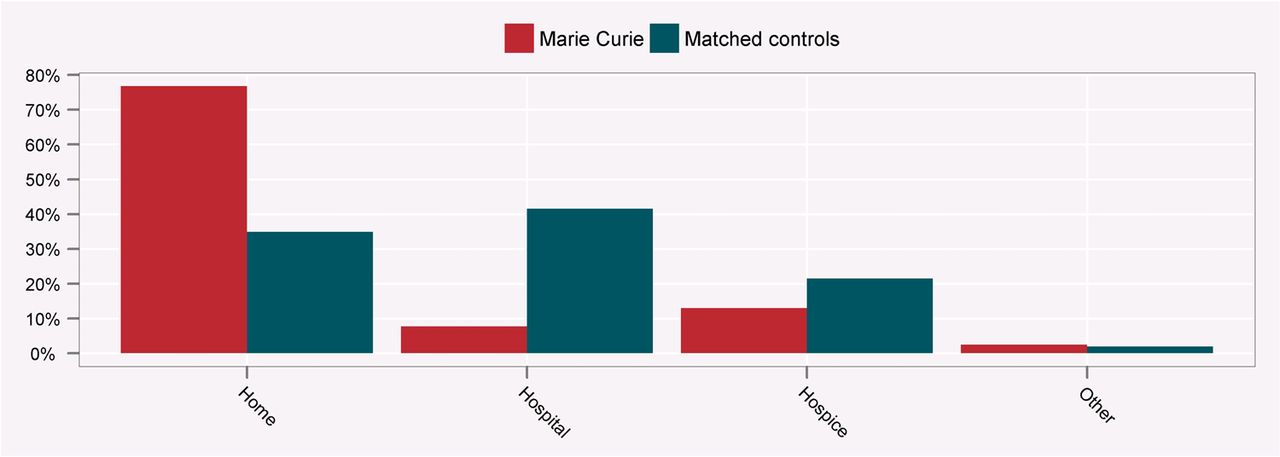
Place of death for intervention patients and matched controls.
Use and costs of hospital care
Intervention patients were significantly less likely than matched controls to use all forms of hospital care after the index date until death (table 2). Only 12% of MCNS patients had an emergency hospital admission after the index date compared with 35% of controls.
Proportion of intervention patients and controls who used hospital care after the index date
Table 3 summarises the average activity per person between the index date and death for intervention patients and matched controls, and the results of the Poisson regression model. The incidence rate ratio showed that across most forms of care intervention patients had between a third and a half of the level of hospital use seen in matched controls.
Hospital activity for intervention patients and matched controls
The costs of hospital care were also significantly lower for intervention patients than matched controls between the index date and death (average unadjusted overall costs £610 per person vs £1750, p<0.001). Significant differences in costs were seen for all types of hospital care (table 4).
Postindex date hospital costs for intervention patients and matched controls
Time from index date until death
Compared with controls, a significantly higher proportion of intervention patients died at home where the time from the index date to death was less than 3 days, compared with those where the index date was 2 weeks or more before death (see online appendix table 5). Figure 2 plots the adjusted difference between cases and controls in the proportion of home deaths with 95% confidence limits, split by the time from the index date to death. The dotted line is the overall adjusted difference between cases and controls.

Adjusted difference between intervention patients and matched controls in proportion of home deaths, by time from index date to death.
There were greater reductions in hospital use and costs for people who started to receive MCNS care longer before death. Compared with matched controls, there was an average crude reduction of 0.09 emergency admissions per person among cases whose index date was 0–2 days before death (incidence rate ratio 0.13, 95% CI 0.10 to 0.16), but more than 0.5 admissions where the index date was at least 2 weeks before death (incidence rate ratio 0.42, 95% CI 0.41 to 0.44). These CIs did not overlap the overall effect (0.19), suggesting that there were subgroup effects. In terms of costs, MCNS patients who started care in the last 2 days before death had an average unadjusted cost reduction compared with controls of £176 (adjusted £154, 95% CI £68 to £239), while for those who started care more than 2 weeks before it was £2291 (adjusted £2252, 95% CI £2181 to £2323). Again, these did not overlap the overall effect (£1113). Online appendix tables 6 and 7 in appendix 1 summarise the differences between the study group and controls, by time from index date to death.
Figure 3 shows the number of emergency admissions per 1000 people by day (relative to death). Each plot is for a different subset of cases and controls, split by the number of days between the index date and death. It shows that the cases and controls were well matched in terms of emergency admissions before the index date, but that emergency admissions stayed static or fell in those who received Marie Curie care, but rose sharply among matched controls in all subsets after the index date.

{kind=link}
{kind=link}
{kind=link}
Number of emergency admissions per 1000 people for cases and controls, by index date.
Sensitivity analysis
The large size of the data sets meant that differences between groups in the endpoints were estimated using methods for independent samples. Sensitivity analysis using conditional logistic regression was done to assess the impact of this modelling strategy on the estimates for the proportional endpoints. The main estimates were conservative; for example, the adjusted ratio for death at home was 6.793 using conditional regression (95% CI 6.468 to 7.134).
Discussion
Compared with a matched control group, people who received home-based nursing care at the end of life were more than twice as likely to die at home (77% vs 35%). They also had significantly lower hospital use for all types of hospital activity. As a consequence, the costs of hospital care for intervention patients were significantly lower than matched controls, with a difference of more than £1100 per person in the period from first receiving a service until death.
Our overall findings are broadly consistent with the existing literature.10–13 15–20 While there have been a number of studies that have investigated the effect of home care on hospital use and place of death, we believe this is the first large-scale retrospective study to use matched controls. Thus, we were able to examine the effects of home-based end-of-life care in routine settings.
The timing of the first contact with the MCNS had a significant impact on the scale of effect. Consistent with an earlier study,23 people whose first home care visit was closer to death were more likely to die at home than those who were in contact with the nursing service for longer. However, compared with controls, much lower levels of hospital activity and costs were seen among intervention patients who were in earlier contact with MCNS.
One explanation for this is that there was a much greater opportunity to influence future hospital use among intervention patients who started care earlier. However, those people also had more time for a hospital admission to occur. Those who only started receiving MCNS care later had managed to remain at home until very close to death, perhaps because their condition was relatively well managed, or because they had access to family or other support. There was a very short window in which they might develop problems necessitating admission.
There are limitations to the analysis. The main threat to validity in a non-randomised study is of systematic differences between intervention and non-intervention patients that are not taken into account (‘confounding’). The control group and intervention patients were well matched on demographic and clinical characteristics, prior hospital utilisation and costs. Therefore, it is unlikely that unobserved confounding could account entirely for the differences in hospital use and place of death seen in this study, given the estimated effect sizes. A randomised controlled trial would have avoided the risk of confounding, but would have limited the applicability of the findings to routine care. In addition, randomised controlled trials can have weaknesses when it is not possible to blind patients and healthcare professionals to treatment allocations.30
Although the intervention patients and control group were well matched on a range of variables, there are likely to be other factors not recorded in routine administrative datasets that influence suitability or preference for home-based care. If these characteristics differed between the groups then this could explain some of the observed differences. For example, the availability of family or other carer support is likely to be an important factor in whether a person can be cared for at home at the end of life. Personal preference for place of care is also a significant determinant. While studies have consistently shown that many people would prefer to die at home,3–5 there is also evidence that a minority would not.31
It is likely that at least some of these hospital cost differences we observed might be accounted for by other services. As well as the nursing service itself, it is also possible that keeping people at home at the end of life would increase demand for other community services, including district nurses, primary care and social care. Future work could explore the impact of end-of-life home care on the broader set of health and care services.32 As well as the direct costs of health and care services, future studies should also take account of the indirect costs to family members and other carers of a person remaining at home at the end of life.
Our analysis did not include the full range of experiences of patients or carers. However, the recent national VOICES survey of recently bereaved people found that care was better for people who died in hospices or at home compared with those who died in hospitals.33
It is very likely that some of the matched controls received inpatient, community or home-based care from an NHS or voluntary organisation, including hospices. Routine information flows do not currently exist to capture much of this activity, and so the extent of it is unknown. However, the aim of this study was to compare intervention patients against those receiving ‘usual care’. As such, ‘usual care’ will reflect a wide range of care pathways.
In an increasingly tight financial climate for public services, there is a drive to identify models of service delivery that can reduce demand for expensive hospital care. A recent review concluded that funding for palliative care in England is complex with significant variation in expenditure and access, meaning thousands of people die annually without access to palliative care that would have benefited them.34 This has led to work to develop a per-patient state-funded system for palliative care. The review suggested that such a change could allow an extra 60 000 people to die at home annually, with significant associated cost savings.
Recognising the potential for different models of care, end-of-life care is a workstream of the government's Quality, Innovation, Productivity and Prevention programme.35 The key aims are to increase the number of people dying in their usual place of residence, and to reduce the number of emergency admissions in the last year of life. Our findings are clearly very relevant to these goals, and suggest that home-based nursing can significantly affect care at the end of life.
Acknowledgments
We are grateful to Michael Cooke and David Bench of Marie Curie Cancer Care for their assistance with the MCNS data used in this study, and Xanthe Hannah of the Information Centre for carrying out the data linkage. We would also like to thank Ian Blunt for providing the costed data used in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendices
Footnotes
-
Contributors XAC, TG and AS led the data analysis. All authors contributed to the design and interpretation of the study and reviewed the manuscript.
-
Funding The study was funded by Marie Curie Cancer Care. The study design was agreed between the Nuffield Trust and Marie Curie Cancer Care. Full control of the analysis, interpretation of the results and publication rights were retained by the Nuffield Trust. Marie Curie Cancer Care were not involved in the preparation of this manuscript nor in the decision to submit for publication.
-
Competing interests Several authors have undertaken evaluative work funded by government or public agencies but these have not created competing interests; there are no other relationships or activities that could appear to have influenced the submitted work.
-
Ethics Approval This study did not require ethics approval as it was based on analysis of existing data using pseudonymised identifiers. Permissions to the use this approach with the NHS IC undertaking data linkage, was obtained from the National Information Governance Board (January 2012). Permission to use mortality data were obtained under the ONS Approved Researcher scheme.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Information available from the corresponding author at martin.bardsley@nuffieldtrust.org.uk.